Finishing the ultrasound QA sessions that we do every week at Stanford, I was reminded about how bedside ultrasound is a tool that helps when resources were limited. If you hadn’t heard, there was an Asiana Airlines plane crash at San Francisco International Airport with over 180 patients requiring medical care, 55+ of which came to Stanford. Luckily, we just added 4 new SonoSite EDGE ultrasound machines to our 4 MTurbos and 3 GE Vscan systems the week before – and they sure were used well! The FAST scan was used as a screening tool and to help prioritize those who would go to the CT scanner. Once, again, it is important to know how to do it and do it well. Our latest insert in the ACEP Ultrasound Section newsletter is below – on the FAST scan – the Cardiac sections. The prior entry was on the FAST scan: The Upper Quadrants ( go here. ) – And Ultrasound Podcast recorded with Cliff Reid about it this week too!
I’ll start with what I’ve said before: “2013 is the YEAR OF ULTRASOUND – and for good reason – there are only a few tools that give us such immediate information that can save a life. The ACEP US Section is the go-to site for everything you want to know about starting an US program, credentialing in ultrasound, the policies and politics, and is the home of SonoGuide – an amazing educational resource for bedside ultrasound, and the EMSONO: Ultrasound Test. It is also where we add our entries for their newsletter that goes over tips and tricks, cases, and all things ultrasound in the news. We recently wrote an article for the ACEP Ultrasound Section Newsletter – which is available for all members of the ACEP US Section – and I highly recommend becoming a member – it’s totally worth it.”
It was a TRUE pleasure to record a podcast recently with Dr. Scott Weingart (aka, my hero) on EMCrit (twitter: EMCrit), and writing this article with our ultrasound fellow, Dr. Viveta Lobo, describes some of what was spoken about.
By Viveta Lobo, MD and Laleh Gharahbaghian, MD, FACEP
As discussed in our last entry, the FAST exam is undoubtedly the most widely used bedside ultrasound application used in emergency medicine. Its incorporation in the ATLS revised protocol, the RUSH exam, and several other published protocols, makes it an invaluable screening tool for intra abdominal injury causing hemoperitoneum, cardiac injury with pericardial effusion, and unexplained hypotension.
We will continue our discussion of the FAST scan by reviewing the cardiac views, and relay some tips and tricks for each. Refer to the previous newsletter for tips onscanning the right upper quadrant (RUQ) and left upper quadrant (LUQ).
The Cardiac Views:
The traditional cardiac view obtained as part of the FAST exam is the subxiphoid view. The main focus of this view in the FAST exam is to evaluate for evidence of cardiac injury by evaluating for pericardial effusion and/or cardiac tamponade. The phased array probe is placed in the subxiphoid space medially, applying pressure to go under the xiphoid process and flattening out the probe while aiming caudally.
Tips for the Subxiphoid View:
 1. Use your liver as an acoustic window.
1. Use your liver as an acoustic window.
 Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
Sound waves will travel through liver to the heart, allowing you to visualize the heart. Often one can even place the probe slightly to the right of the xiphoid process, to allow for better liver visualization, and then adjust your depth to be able to look past the liver to the heart. Without the liver in view, gas scatter will affect your image acquisition.
2. Visualize both the inferior and superior pericardial borders, to completely evaluate for pericardial effusion or, rarely, loculated pericardial effusions. It is possible for one area to have pericardial effusion and not the other. Click Here for a Video.
3. Have the patient take a deep breath and hold it. When you notice that the heart is far from the probe, and you find yourself adjusting your depth to more than 20cm, having your patient take a deep breath will lower the heart closer to the probe, improving visualization. Click Here for a Video.

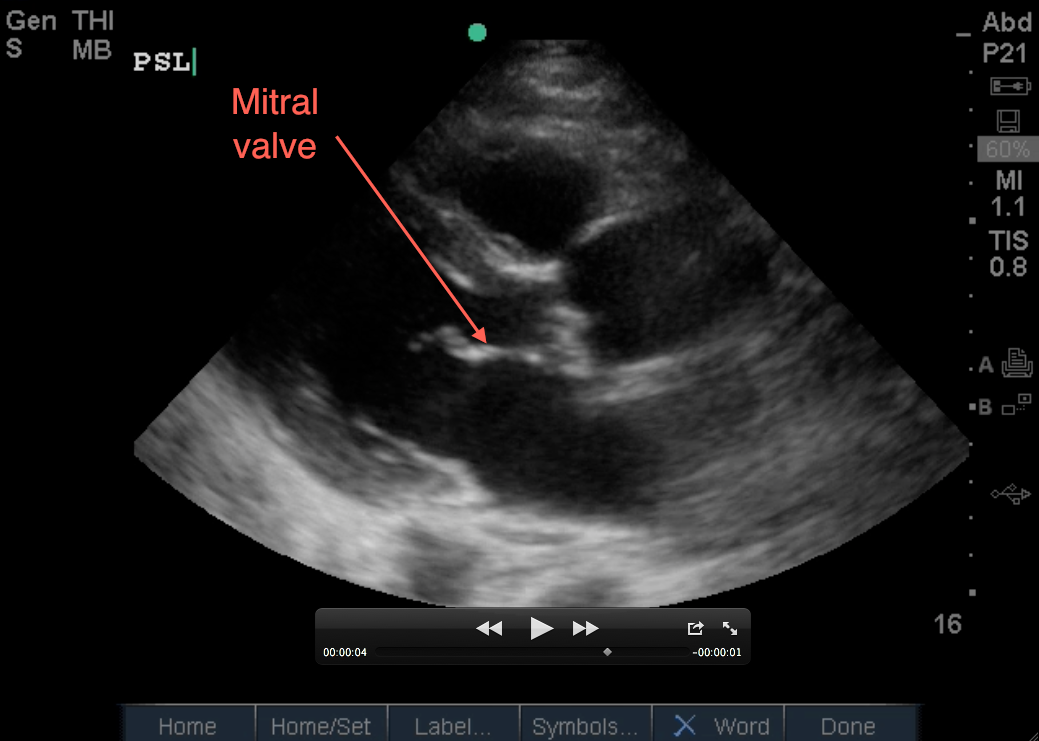
Despite the subxiphoid view being the traditional view for the FAST exam, the parasternal long view is becoming more of the ‘go-to’ window to evaluate for pericardial effusion. This may be due to several very relevant clinical factors: You simply cannot get a good subxiphoid view. An injury, foreign body, or abdominal pain does not allow for subxiphoid probe placement/pressure. Or you can differentiate pericardial fluid from pleural fluid in the parasternal long view.
Tips for Parasternal Long View:
As far as patient positioning, if you’ve already evaluated the RUQ and LUQ (so as to not affect free fluid evaluation) and the patient is able to turn into a left lateral decubitus position, it will help bring the heart closer to the chest wall for visualization. This can be difficult, or impossible, in trauma patients, so the below tips may help:
 1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.
1. Start high and start medial – Place your phased array probe just next to the sternum, starting just under the clavicle. If you don’t see the heart there, slide down a rib space, and fan through that space to find the heart. Continue sliding down rib spaces, until you find it.
2. Slowly change the angle of your probe (up and down) when you’re assessing each rib space as described above. ‘Slowly’ is the key word here. If you’re angling downward too much in a rib space and see the PSL heart, you may need to just slide down a rib space. If that makes the image worse, slide back up.
3. Slowly rotate your probe while keeping the angle described above (clockwise/counterclockwise depending on whether you use the right shoulder or the left hip to direct your probe marker). Rotate until you visualize the longitudinal view of the left side of the heart.
4. Slide your probe medially/laterally only if you need to in order to center the aortic and mitral valves on your screen.
5. Ensure adequate depth in order to distinguish a left sided pleural effusion from a pericardial effusion. This will allow visualization of the descending thoracic aorta seen in its transverse view just deep to the heart, which is your landmark in differentiating pleural effusion from pericardial effusion. Pleural effusion will travel posterior to the aorta while pericardial effusion will travel anterior to it (and possibly circumferentially around the heart).

 Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.
Lastly, it can be very difficult in both subxiphoid and parasternal long views to differentiate epicardial fat pad from pericardial effusion. One tip: epicardial fat is seen anteriorly and has echogenicity within it, while pericardial effusion is seen posteriorly or inferiorly and is anechoic, but can travel anteriorly if large enough to become a circumferential pericardial fluid collection. Despite this tip, clinical correlation is needed.
Look out for Part 3 of the FAST Exam: The Pelvis, in the next newsletter. Until next time, happy scanning!
For a set of links to online education in bedside ultrasound, go here. Another post on Social Media in EM Ultrasound and the amazing tools out there to learn it for free, go here.”
References
1. Ma OJ, Mateer JR, Ogata M, et al. Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma. 1995; 38:879-85.
2. Wherrett LJ, Boulanger BR, McLellan BA, et al. Hypotension after blunt abdominal trauma: the role of emergent abdominal sonography in surgical triage. J Trauma. 1996;41:815-20.
3. Schiavone WA, Ghumrawi BK, Catalano DR, et al. The use of echocardiography in the emergency management of nonpenetraing traumatic cardiac rupture. Ann Emerg Med. 1991;20:1248-50.
4. Rozycki GS, Feliciano DV, Ochsner MG, et al. The role of ultrasound in patients with possible penetrating cardiac wounds: a prospective multicenter study. J Trauma. 1999;46:543-52.