
In a recent issue of the Journal of Ultrasound through AIUM, Weekes et al. (and Kendall et al in AM J EM) talk about a hot topic that emergency and critical care physicians hold dear to them – the EPSS , or E-point septal separation – the minimal distance between the anterior mitral valve leaflet and the interventricular septum in the parasternal long view of the cardiac echo during diastole using M-Mode. Now, EPSS is not a part of point of care echo right now (i know, phew!), but there are conversations about whether it should be. The reason is because it is thought that EPSS is a good tool for LV function delineation, possibly better than simple visualization, despite knowing the risks of underestimating ejection fraction due to endocardial output limitations (see below). …Yeah, I know, that’s a lot of words and it took me a year to really understand what the above meant. So, let’s talk about it…especially as it is included in the updated RUSH protocol by Seif, Perera, et al.
EPSS by echo has even been compared to cardiac MRI for LV function recently. And, Dr. Mike Stone and friends did a study last year with regard to EPSS compared to qualitative LV function, stating: “Dyspneic patients with acute decompensated heart failure (ADHF) often present to the emergency department (ED), and emergency physicians (EPs) must act quickly and accurately to evaluate and diagnose patients with ADHF. Traditionally, key components of the patient’s history, physical examination, electrocardiography, and chest radiography are used to diagnose ADHF. However, no single test is highly accurate, and even with the incorporation of B-type natriuretic peptide levels, the diagnosis of ADHF in a dyspneic patient in the ED can be a challenge. Additional modalities that allow prompt and accurate diagnosis of ADHF would be of clinical utility, and estimation of left ventricle ejection fraction (LVEF) using point-of-care ultrasound has been the focus of prior research” showing that EPSS is a good tool compared to qualitative LVEF visualization. EM News folks also highlighted EPSS in a recent entry.
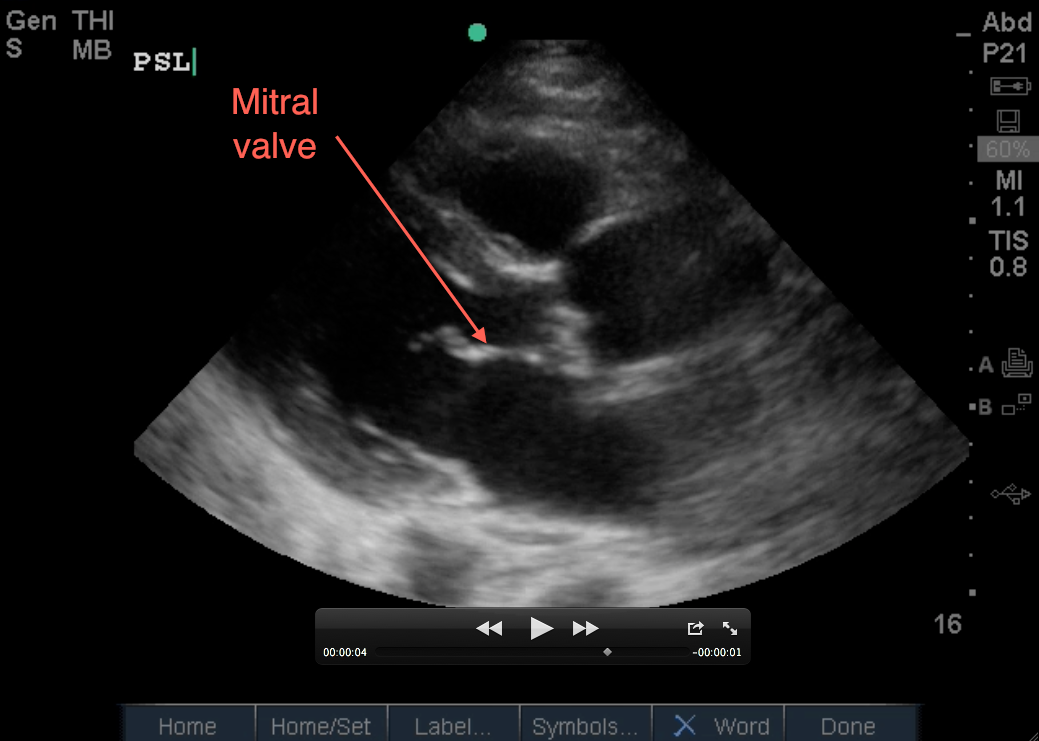
Now, lets talk a bit about the anatomy and physiology about this before we talk about the study. The mitral valve has an anterior leaflet and a posterior leaflet. You can see the mitral valve open and close in the parasternal long view of the heart. the below picture indicates the anterior leaflet:
Using the Cardiovscular Institute’s diagrams, we can see the functioning of the mitral valve during systole and diastole in relation to the EKG, with every movement /peaks delineated with a letter ….one of them being “e” (where E of EPSS comes from):


…and in relation to the EKG on M-mode on the PSL view (aka motion mode – basically visualizing the motion of objects in time).


EPSS of >7mm is thought to be an indication of poor LV function. Some use 1cm as the mark to increase their sensitivity for low ejection fraction. So, you can see that it should be a good indicator of LV function.
Fractional shortening (FS), however, is….(LVEDd-LVESd) / LVEDd expressed as a percentage. Placing the M-mode cursor across the LV just beyond the mitral valve leaflets, a tracing is shown whose measurements of the LV chamber diameter in both systole and diastole can illustrate FS, or LV contractility (not ejection fraction as it is not a volume measurement). Normal FS being 30-45%. For a complete description of these terms go here – a great overview by ICU Sonography – and here – a simpler way to understand the measurements through the Stanford ICU website. The updated RUSH protocol, also explains this well, with images from their most recent publication below:
Hyperdynamic/hypercontractile: FS >45%

Abnormal: hypocontractile LV: FS<30%

So, the study was a prospective study, thankfully, and seemed to really want EPSS to be good for LV function, but it looks like it’s not as good as we think:
Abstract: “Objectives Rapid bedside assessment of left ventricular (LV) function can aid in the evaluation of the critically ill patient and guide clinical management. Our primary hypothesis was that mitral valve E-point septal separation measurements would correlate with contemporaneous fractional shortening measurements of LV systolic function when performed by emergency physicians. Our secondary hypothesis was that E-point septal separation as a continuous variable would predict fractional shortening using a linear regression model.
Methods We studied a prospective convenience sample of patients undergoing a sequence of LV systolic function measurements during a 3-month period at a suburban academic emergency department with a census of 114,000 patients. The sample included adult emergency department patients who were determined by the treating emergency physician to have 1 or more clinical indications for bedside LV systolic function assessment. Investigators performed bedside M-mode cardiac sonographic measurements of fractional shortening and E-point septal separation using the parasternal long-axis window. The sequence of LV systolic function measurements was randomized.
Results A total of 103 patients were enrolled. The Pearson correlation coefficient for E-point septal separation and fractional shortening measurements was –0.59 (P< .0001). Linear regression analysis performed for E-point septal separation with fractional shortening as the dependent variable yielded an R2 value of 0.35.
Conclusions E-point septal separation and fractional shortening measurements had a moderate negative correlation. E-point septal separation, when used as a continuous variable in a linear regression model, did not reliably predict fractional shortening.”
The limitations of EPSS as discussed in Stone’s paper:
Valvular diseases that restrict anterior mitral leaflet motion ( mitral stenosis, aortic insufficiency) – will exaggerate EPSS.
Asymmetric septal hypertrophy,
Severe left ventricular hypertrophy,
Discrete proximal septal thickening (sigmoid septum) can lead to small
estimates of EPSS.
Failure to obtain a true parasternal long-axis view may result in falsely elevated
EPSS measurements due to a tangential measurement from mitral valve leaflet to septal wall.
….At the end of the day, my opinion -> just visualizing the LV contractility, as long as you have a good PSL and PSS long view, and you’ve seen enough to know normal versus abnormal, is good enough for me!

Hello. EPSS is a very simple measurement that must be put in context. In my point of view is not the panacea and maybe it is a good indicator of LV dilation more than LV systolic function. It is well studied the correlation of MAPSE (averaged in two or 4 mitral annulus points) with LV EF and I don´t know why it is not used in everyday practice and put in rapid ultrasound protocols, it is really simple to do, you only need a A4C view, that, in critical care patients is more obtainable than PLAX.
Best
PB
Critical care physician from Argentina
PB – thanks for your comment, and there are quite a few ways for objective data for contractility, thankfully – some quicker than others, which is what we need in critical patients where time is of the essence. EPSS has come under fire, and rightfully so, as it is not perfect. Fractional shortening has gotten more love but again require an appropriate sectioning of the parasternal view. Apical views can be difficult to obtain, especially in patients who cannot turn to their side in resuscitation, but another method that should be studied.